Complications of endourological procedures and their treatment
Accepted: October 21, 2020
Supplementary Files: 143
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Endourological treatment for urinary stones and other obstructive urinary tract diseases is minimally invasive but in some cases it involves serious complications. This collection of cases describes some complications of endourological procedures and how they were treated.
Case 1: A case of right ultrasound-guided percutaneous nephrostomy found to be misplaced in the inferior vena cava. The case was safely managed, but it showed that ultrasound guidance alone may be insufficient so it is recommended that percutaneous nephrostomy should be always placed under fluoroscopic control, either alone or in combination with ultrasound guidance.
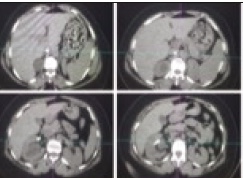
Case 2: A case of renal subcapsular hematoma occurring on retrograde intrarenal surgery at high perfusion pressure. The hematoma was drained under combined ultrasonic and radiological guidance. Post treatment recovery was uneventful. Large stone size, severe ipsilateral hydronephrosis, long operation time, higher hydrostatic pressure of the irrigating solution and low ureteral wall compliance are supposed to be risks factors associated with renal subcapsular formation. Management strategy should be tailored to patient’s clinical conditions. In hemodynamically stable patients, large hematoma drainage is recommended to prevent further complications and favours early recovery.
Case 3: A case of double J stent fracture discovered one month after the insertion to relieve obstruction from a 1 cm stone in the right proximal ureter. The distal fragment of the stent was removed by cystoscopy while the proximal fragment was removed by semirigid ureteroscopy in two sessions due to fever and extensive calcification. Case 4: A mini-invasive technique for transurethral replacement of completely encrusted urinary stents in female patients. This technique allows the interventional radiologist to replace obstructed urinary stents by avoiding more invasive and traumatic urological procedures with sedation.




How to Cite
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
