Abstract (extended summary by S. Ricci)
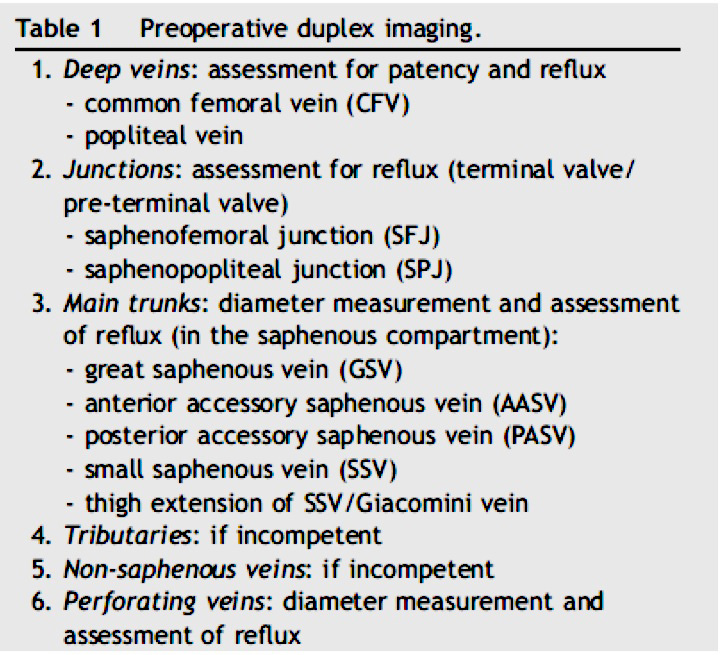
The aim of this paper is to summarize the best practice for venous duplex ultrasound investigation (DUS) examination of the lower limbs after treatment. Parts of this paper have been taken from the limited evidence available in the literature and was agreed upon by a group of experts who regularly use this technology. DUS evaluation after treatment must take into consideration the pre-treatment assessment. Patients have different profiles of anatomic and hemodynamic superficial venous insufficiency. Clear documentation of pre-treatment clinical features and DUS findings is, therefore, essential as these may influence the interpretation of post treatment results and expectations The minimum requirements for pre-treatment DUS assessment are described in Table 1.
When assessing superficial veins, patients should be examined, where possible, in a standing position in order to standardize measurement of the venous diameter and reflux. If obesity or other cardio-respiratory conditions make this impractical, it is vital that the position used is adopted for any follow-up imaging. The diameter should be measured in transverse view 3 cm below the saphenofemoral junction (SFJ), at mid-thigh level, at the knee and also at mid-calf level; the outer diameter should also be measured (including the vein wall) for comparison with the postoperative diameter after endovenous ablation (EVA). Similarly, these modalities should be used for the anterior accessory saphenous vein (AASV) and for the small saphenous vein (SSV).
To detect the presence of reflux, a pressure gradient in the venous system by a Valsalva maneuver (high pressure in the venous system) is required, or this should be achieved by a compression /release maneuver (low pressure in the distal venous system during release).
At the level of the SFJ, the combination of these two maneuvers is essential to assess the state of the terminal valve (TV) of the great saphenous vein (GSV). TV and PTV hemodynamics are best assessed through the combined use of color flow and Doppler, with the sample volume placed above each valve to test for the presence or absence of reflux. The inguinal lymph node area should be studied, particularly in patients with recurrent varicose veins and also for veins that are part of the abdominal/pelvic venous network.
Any treatment should be recorded in sufficient detail as to allow an informed DUS follow up.
The timing of outcome assessment should be classified as immediate (1-4 weeks), short-term (1 year), midterm (2-3 years) and long-term (5 years or more).
Following surgical treatment, DUS imaging should focus on the saphenous junctions (SFJ and SPJ) and keep track of the stripped saphenous trunk (GSV, AASV or SSV). In recurrences, all escape points should be documented to highlight either reflux following a Valsalva, which indicates that there is a change of compartment or escape points (connection with the deep veins) or that a reflux which is generated only by a compression/release maneuver (not by Valsalva) is not linked to an escape points but takes place only in the superficial network.
Neovascularization is defined as the presence of multiple new, small tortuous veins in anatomic proximity to a previous venous intervention. Neovascular veins may show reflux with a Valsalva maneuver (escape points usually in the SFJ area) and/or during release after calf compression (filling from the subcutaneous abdominal venous network). If they are seen to be associated with a lymph node, they are described as a lymph node vein network.
The largest diameter of the vein(s) of the vascular network in the groin should be measured.
If GSV ligation has been performed at a distance from the CFV (low ligation) instead of flush to the SFJ level, a residual stump may be seen. Reflux from the residual stump can connect with a residual AASV or other varices and should be assessed on DUS. When the terminal valve is competent, the stump receives inflow from its tributaries that normally drain into the SFJ. This may be found after selective stripping of the GSV trunk without a flush ligation, preserving the saphenofemoral confluence. In patients who have had surgical stripping, revascularization of the strip-track (the presence of multiple convoluted channels in the track of the previously stripped GSV) may be found.
The AASV should be examined along its course as it is often involved in recurrence after GSV stripping.
After SSV surgery at the level of the SPJ, DUS findings are comparable to those at the SFJ after GSV surgery.
Anatomy and hemodynamics of the popliteal fossa complex vary in SPJ. It is, therefore, particularly important to have details about the pre-operative anatomic and hemodynamic situation, as well as of the procedure performed. Similar to the groin, the neovascular veins may connect directly to the popliteal vein, or they may connect with incompetent veins in the posterior thigh. An incompetent residual stump with or without reflux is frequently seen after SSV surgery. This may be due to the great variation in SPJ level.
In primary venous insufficiency, perforators that transmit part or all the reflux from the superficial into the deep venous system are described as re-entry perforators. After saphenous stripping and phlebectomy, they mainly show normal inward flow and a diameter reduction at short- and mid-term follow up. Conversely, many cases of recurrent varices can be related to more or less underdiagnosed incompetent perforators.
On the back of the thigh, varicose veins may receive reflux from a gluteal plexus or vulvar/perineal veins, and are often related to pelvic vein incompetence. By carefully tracing these veins upwards while eliciting reflux with a distal compression/release maneuver, it is possible to detect their origin.
After endovenous treatment of the GSV with laser, RFA or foam, the terminal part of the GSV usually remains open
allowing one or more tributaries of the SFJ to drain; under 3 cm in length is considered to be within normal limits. Protrusion of a thrombus into the lumen of the CFV is very unusual (<1%) and should always be considered a pathological finding. Persistence or reappearance of reflux at the SFJ and/or at the level of the saphenous stump is always considered pathological. Usually, no connection with any visible varicose veins is detectable at short-term follow up. Any varicose veins in connection with the stump should be imaged.
Treated veins (GSV, SSV and/or AASV) should be assessed by their compressibility, as well as using color flow.
The sonographic appearance of the obliterated vein will depend on the stage of post-treatment evolution.
Subsequent obliteration is characterized by a progressive reduction in vein diameter; this is often not homogeneous
over the length of the treated vein. In the final stage of fibrotic transformation the vein may disappear
completely on DUS imaging or is transformed into a fibrous cord that may be visible as a hyperechogenic tract in the saphenous compartment. It usually takes 6-12 months before the vein can no longer be seen at all.
The presence of reflux following a Valsalva or compression/release maneuvre is pathological.
Reflux distribution in the saphenous trunk and/or tributaries, together with the re-entry or refluxing perforators should be recorded. Antegrade flow without reflux can sometimes be demonstrated in a partially or completely patent residual GSV trunk.
Changes in the SPJ and SSV are similar to those of the SFJ and GSV and should, therefore, be reported in the same way. At the SPJ, proximal tributaries may remain patent, particularly any extension of the SSV into the thigh or the Giacomini vein.
Perforating veins that remain patent should be reassessed to compare the normal inward flow and pathological outward flow in order to determine the net flow. The latter is obtained by comparing mutually pulsed Doppler curves of inward and outward flow during distal compression and release.
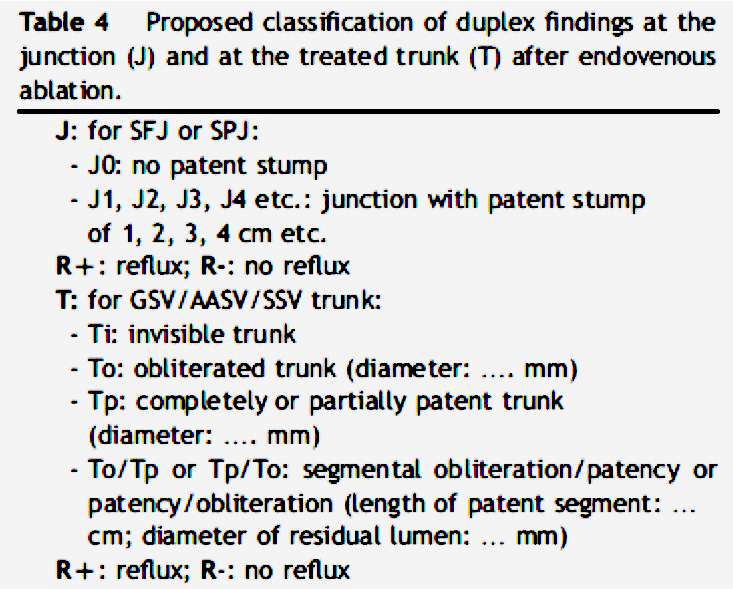
DUS data are objective and reproducible, particularly when obtained and reported using standard methodology that facilitates a reliable collection of serial data in individual patients and in patient groups. Results after EVA should be standardized on the basis of scientific studies. The authors propose a classification (Table 4) that allows a precise analysis of the results after EVA in order to compare different techniques and introduce a standard DUS assessment of outcomes following any EVA procedure.
Using a single grading system for clinical outcome that combines symptom scores, clinical findings and DUS findings to define the global outcome will not produce a coherent classification system, as the relative importance of individual variables may differ. It is, therefore, appropriate to report separately on clinical outcome parameters and DUS findings in all patients included in prospective studies.
|