
Different diagnostic strategies for different settings
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 25 February 2021
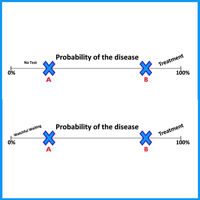
Diagnostic strategies should always take into consideration the setting in which they are administered. The predictive value, positive or negative of a clinical sign or diagnostic test has a different weight in family medicine than in the hospital setting. Many tests have not been formally evaluated in primary care; unfortunately, very often low prevalence settings are used to conduct screening in these populations, and often result in unrealistically high prevalence estimates for chronic disease and these results are then used to conclude that General Practitioners are not good at detecting diseases. In primary care, the prevalence and incidence of disease differs from what appears in the hospital setting, and severe disease occurs less frequently in general practice than in hospital because there is no preventive selection. This requires a specific probability-based decision-making process, based by the knowledge of patients and the community. In primary care, the diagnostic strategy should begin with complaints and symptoms and address uncertainty and complexity, using step-by-step strategies, including watchful waiting, presumptive symptomatic treatment, and focusing on low-tech strategies.
Downloads
Shaneyfelt T. Pyramids are guides not rules: the evolution of the evidence pyramid. Evid Based Med 2016;21:121-2. DOI: https://doi.org/10.1136/ebmed-2016-110498
Parikh R, Parikh S, Arun E, Thomas R. Likelihood ratios: clinical application in day-to-day practice. Indian J Ophthalmol 2009;57:217. DOI: https://doi.org/10.4103/0301-4738.49397
Moritz S, Ferahli S, Naber D. Memory and attention performance in psychiatric patients: lack of correspondence between clinician-rated and patient-rated functioning with neuropsychological test results. J Int Neuropsychol Soc 2004;10:623-33. DOI: https://doi.org/10.1017/S1355617704104153
Petrazzuoli F, Vestberg S, Midlöv P, et al. Brief cognitive tests used in primary care cannot accurately differentiate mild cognitive impairment from subjective cognitive decline. J Alzheim Dis 2020:1-11. DOI: https://doi.org/10.3233/JAD-191191
Hurford IM, Marder SR, Keefe RS, et al. A brief cognitive assessment tool for schizophrenia: construction of a tool for clinicians. Schizophr Bull 2011;37:538-45. DOI: https://doi.org/10.1093/schbul/sbp095
Mathers N, Hodgkin P. The gatekeeper and the wizard: a fairy tale. BMJ 1989;298:172. DOI: https://doi.org/10.1136/bmj.298.6667.172
Sackett DL, Haynes RB, Tugwell P. Clinical epidemiology: a basic science for clinical medicine. Little: Brown and Company; 1985.
Linn S, Grunau PD. New patient-oriented summary measure of net total gain in certainty for dichotomous diagnostic tests. Epidemiol Perspect Innovat 2006;3:11. DOI: https://doi.org/10.1186/1742-5573-3-11
Koepsell TD, Connell FA. Measures of gain in certainty from a diagnostic test. Am J Epidemiol 1985;121:744-53. DOI: https://doi.org/10.1093/aje/121.5.744
Salmi LR, McGill U. Re: “Measures of gain in certainty from a diagnostic test”. Am J Epidemiol 1986;123:1121-2. DOI: https://doi.org/10.1093/oxfordjournals.aje.a114343
Irving G, Holden J. The time-efficiency principle: time as the key diagnostic strategy in primary care. Family Pract 2013;30:386-9. DOI: https://doi.org/10.1093/fampra/cmt007
Almond SC, Summerton N. Diagnosis in general practice. Test of time. BMJ 2009;338:b1878. DOI: https://doi.org/10.1136/bmj.b1878
Crossley T. I Don’t know what it is but I don’t think it’s serious: confidence and decisiveness in primary care. London: Royal College of General Practitioners; 2008.
Hart JT. The political economy of health care: a clinical perspective; 2006. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2465620/
Sox Jr HC, Hickman DH, Marton KI, et al. Using the patient’s history to estimate the probability of coronary artery disease: a comparison of primary care and referral practices. Am J Med 1990;89:7-14. DOI: https://doi.org/10.1016/0002-9343(90)90090-Z
Soler J-K, Okkes I, Wood M, Lamberts H. The coming of age of ICPC: celebrating the 21st birthday of the International Classification of Primary Care. Family Pract 2008;25:312-7. DOI: https://doi.org/10.1093/fampra/cmn028
Schneider A, Löwe B, Barie S, et al. How do primary care doctors deal with uncertainty in making diagnostic decisions? The development of the ‘Dealing with Uncertainty Questionnaire’(DUQ). J Evaluat Clin Pract 2010;16:431-7. DOI: https://doi.org/10.1111/j.1365-2753.2010.01464.x
Hamilton W, Sharp D. Diagnosis of colorectal cancer in primary care: the evidence base for guidelines. Family Pract 2004;21:99-106. DOI: https://doi.org/10.1093/fampra/cmh121
Howie J. Diagnosis--the Achilles heel? J R Coll General Pract 1972;22:310.
Jamoulle M. Quaternary prevention: first, do not harm. Rev Brasil Med Fam Comun 2015;10:1-3. DOI: https://doi.org/10.5712/rbmfc10(35)1064
Mold JW, Stein HF. The cascade effect in the clinical care of patients. Mass Medical Soc 1986;314:512-4.
Starfield B. William Pickles Lecture. Primary and specialty care interfaces: the imperative of disease continuity. Br J General Pract 2003;53:723.
Stange KC, Ferrer RL. The paradox of primary care. Ann Family Med 2009;7:293-9. DOI: https://doi.org/10.1370/afm.1023
Irving G, Reeve J. Do GPs really provide 47 minutes a year for the patient? Br J General Pract 2012;62:404-5. DOI: https://doi.org/10.3399/bjgp12X653499
Hummers-Pradier E, Beyer M, Chevallier P, et al. The research agenda for general practice/family medicine and primary health care in Europe. Part 1. Background and methodology 1. Eur J General Pract 2009;15:243-50. DOI: https://doi.org/10.3109/13814780903452184
Hill AP, Freeman GK. Promoting continuity of care in general practice. London: Royal College of General Practitioners; 2011.
Rogers E. Diffusion of innovations, 5th edn. New York, NY: Free Press; 2003.
Studdert DM, Mello MM, Sage WM, et al. Defensive medicine among high-risk specialist physicians in a volatile malpractice environment. JAMA 2005;293:2609-17. DOI: https://doi.org/10.1001/jama.293.21.2609
How to Cite
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.