
Can Left ventricular outflow tract aortic velocity time integral guide fluid resuscitation in septic patients? - A case report
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 25 August 2020
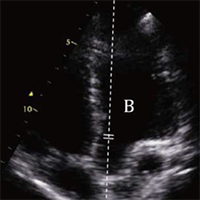
Hemodynamic monitoring of unstable patients is an everyday issue for Emergency Physicians (EP). Considering the difficulty, in Emergency Department (ED) settings, to assess invasively Stroke Volume (SV), Cardiac Output (CO) and Peripheral Vascular Resistance (PVR), EP should be familiar with non-invasive, easy and reproducible methods that can estimate these parameters. The use of Left Ventricular Outflow Tract aortic Velocity Time Integral (LVOT-VTI) with echocardiography, as estimate of SV, integrated with inferior vena cava collapse index and clinical examination could give the opportunity to non-invasively understand at which point of an ideal cardiac output/central venous pressure relation (according to the Frank Starling law) the patient is situated. In this case report we describe a septic patient accessing the ED with both respiratory and cardiac failure, and we show that the use of aortic LVOT-VTI is an easy and reproducible approach to understand cardiac hemodynamic in scenarios involving multiple pathologic mechanisms.
Downloads
De Backer D, Cholley P, Slama M, Vieillard-Baron A, Vignon P. Hemodynamic monitoring using echocardiography in the critically ill; Springer; 2011, DOI: https://doi.org/10.1007/978-3-540-87956-5
Malbrain M, Van Regenmortel N, Saugel B. et al. Principles of fluid management and stew-ardship in septic shock: it is time to consider the four D’s and the four phases of fluid thera-py. Ann. Intensive Care 2018; 8, 66 DOI: https://doi.org/10.1186/s13613-018-0402-x
Magder S. The meaning of blood pressure. Crit Care. 2018; 22: 257 DOI: https://doi.org/10.1186/s13054-018-2171-1
Pinsky MR, Teboul JL, Vincent JL. Hemodynamic Monitoring; Springer; 2019 DOI: https://doi.org/10.1007/978-3-319-69269-2
Viellard-Baron A, Millington SJ, Sanfilippo, Chew FM et al. A decade of progress in critical care echocardiography: a narrative review Intensive Care Med 2019; 45:770-88 DOI: https://doi.org/10.1007/s00134-019-05604-2
Pinsky MR, Payen D Functional hemodynamic monitoring Crit Care 2005; 9: 566-72 DOI: https://doi.org/10.1186/cc3927
Cikes M, Solomon SD. Beyond ejection fraction: an integrative approach for assessment of cardiac structure and function in heart failure European Heart Journal 2015; 37: 1642-50 DOI: https://doi.org/10.1093/eurheartj/ehv510
Cholley B. Echocardiography in the intensive care unit: beyond “eyeballing”. A plea for the broader use of the aortic velocity-time integral measurement Intensive Care Med 2019; 45: 898-901
Vieillard-Baron A, Caille V, Charron C, Belliard G et al. Actual incidence of global left ven-tricular hypokinesia in adult septic shock. Crit Care Med 2008; 36:1701-06 DOI: https://doi.org/10.1097/CCM.0b013e318174db05
McLean S.A. Down but not out: myocardial depression in sepsis. Crit Care 2012; 16, 132 DOI: https://doi.org/10.1186/cc11367
How to Cite
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.

