
Effect of adding dexmedetomidine or remifentanil to thiopental in patients with mood disorder candidate for electroconvulsive therapy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 4 August 2020
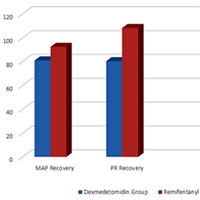
Electroconvulsive therapy (ECT) is one of the appropriate treatments for many neuropsychiatric patients, especially those with mood disorders. Short-term complications of ECT include agitation and postictal. In this study, we compared the addition of dexmedetomidine or remifentanil to thiopental as the main anaesthetic used in ECT. In this double-blind randomised clinical trial, 90 patients with mood disorders (candidates for ECT) were divided into two groups based on their therapy: dexmedetomidine or remifentanil. In the first group (DG), patients were slowly injected intravenously with 0.5 μg/kg dexmedetomidine before induction of anesthesia. In the second group (GR), 100 μg of remifentanil was slowly injected intravenously.In addition, we collected demographic information such as respiratory rate, heart pulse rate, seizure time, mean of arterial blood pressure, recovery duration and the oxygen arterial saturation recorded after recovery. Data obtained were analysed by use of statistical software, SPSS-23. The mean age of both groups was approximately 37 years with the majority being men. There was no significant difference between the two groups in terms of age and sex, blood pressure, heart rate, duration of seizures and arterial oxygen saturation before ECT. The mean blood pressure and heart rate in the recovery group were lower in the dexmedetomidine group than in the remifentanil group and the hemodynamics in the dexmedetomidine group were more stable. The recovery time in the dexmedetomidine group was longer than that of the remifentanil group (p = 0.001). Both groups had approximately the same satisfaction and the rate of agitation after ECT was the same. Both remifentanil and dexmedetomidine as adjuvants lead to a decrease in patients' post-ECT hyperdynamic responses. In our study, we demonstrated that the effect of dexmedetomidine is greater than remifentanil. On the other hand, neither dexmedetomidine nor remifentanil had a negative effect on seizure duration, but dexmedetomidine significantly prolonged recovery time, when compared to remifentanil.
Downloads
Bayati A, Beigi M, Salehi M. Depression prevalence and related factors in Iranian students. Pak J Biol Sci. 2009; 12: 1371-5. DOI: https://doi.org/10.3923/pjbs.2009.1371.1375
Kessler RC1, Aguilar-Gaxiola S, Alonso J,et al.The global burden of mental disorders: an update from the WHO World Mental Health (WMH) surveys. Epidemiol Psichiatr Soc. 2009;18:23-33. DOI: https://doi.org/10.1017/S1121189X00001421
Aksay SS, Bumb JM, Jank C, et al. Serum lipid profile changes after successful treatment with electroconvulsive therapy in major depression: A prospective pilot trial. J Affect Disord. 2016; 18: 85-8. DOI: https://doi.org/10.1016/j.jad.2015.09.037
Moshiri E, Modir H, Bagheri N,et al. Premedication effect of dexmedetomidine and alfentanil on seizure time, recovery duration, and hemodynamic responses in electroconvulsive therapy. Ann Card Anaesth. 2016;19:263-8. DOI: https://doi.org/10.4103/0971-9784.179618
Aksay SS, Bumb JM, Remennik D,et al. Dexmedetomidine for the management of postictal agitation after electroconvulsive therapy with S-ketamine anesthesia. Neuropsychiatr Dis Treat. 2017 ;13:1389-1394. DOI: https://doi.org/10.2147/NDT.S134751
Lisanby SH. Electroconvulsive therapy for depression. N Engl J Med. 2007; 357: 1939-1945. DOI: https://doi.org/10.1056/NEJMct075234
Recart A, Rawal S, White PF,et al. The Effect of Remifentanil on Seizure Duration and Acute Hemodynamic Responses to Electroconvulsive Therapy. Anesh Analg. 2003; 98: 1047-50. DOI: https://doi.org/10.1213/01.ANE.0000054002.65040.B3
Augoustides JG, Greenblatt E, Abbas MA, et al. Clinical Approach to agitation after electroconvulsive therapy, a case report and literature review. JECT. 2002; 18: 213-217. DOI: https://doi.org/10.1097/00124509-200212000-00009
Shams T, El Masry R. Ketofol – Dexmedetomidine combination in ECT : A punch for depression and agitation. Indian J Anaesth. 2014; 58: 275-80. DOI: https://doi.org/10.4103/0019-5049.135037
Wijeysundera DN, Bender JS, Beattie WS. Alpha-2 adrenergic agonists for the preventio of cardiac complication among patients undergoing surgery. Cochrane Database Syst Rev. 2009; 4(11): 4126-31.
Singh AK, Kumar A, Kumar A,et al. A Comparison of Intrathecal Dexmedetomidine and Neostigmine as Adjuvant to Ropivacaine for Lower Limb Surgeries: A Double-blind Randomized Controlled Study. Anesth Essays Res. 2017;11:987-992. DOI: https://doi.org/10.4103/aer.AER_62_17
Anderson J GU, Siegel H, Dahl J, et al. Does Dexmedetomidine Have a Perineural Mechanism of Action When Used as an Adjuvant to Ropivacaine?: A Paired, Blinded, Randomized Trial in Healthy Volunteer. Anesthesiol 2017; 12: 66-73. DOI: https://doi.org/10.1097/ALN.0000000000001429
Dubovsky SL, Thomas M J. Nicardipine improves the antidepressant action of ECT but does not improve cognition. Mar. 2001; 17: 3-10.
Li X, Tan F, Jian CJ, et al. Effects of small dose dexmedetomidine on hyperdynamic responses to electroconvulsive therapy. J Chin Med Assoc. 2017;80:476-481. DOI: https://doi.org/10.1016/j.jcma.2017.02.008
Salehi B, Mohammadbeigi A, Kamali AR, et al. Impact comparison of ketamine and sodium thiopental on anesthesia during electroconvulsive therapy in major depression patients with drug-resistant; a double-blind randomized clinical trial; Ann Cardiac An aesthesia. 2015 ;4: 486-490. DOI: https://doi.org/10.4103/0971-9784.166444
Bzthidsefo D. Dexmedetomiane biunts acute hyperdynamic responses to electroconvulsive therapy without altering seizure duration. Acta Anaesthesiol Scand. 2008; 52: 302-6. DOI: https://doi.org/10.1111/j.1399-6576.2007.01462.x
Kashaki M, Masoudi Samghabadi F, Bordbar A.Effect of Fortification of Breast Milk in Conjugation with Protein Supplement on Neurodevelopment of Preterm Low Birth Weight Infants at 3 Years. Med Arch. 2019 ; 73(5): 344–350. DOI: https://doi.org/10.5455/medarh.2019.73.344-350
KashakiM, MazouriA, BordbarA, e al. Effect of Protein Supplementation on the Growth of Infants Weighing Less than 1,000 Grams Hospitalized on the Neonatal Intensive Care Unit of Akbar Abadi Hospital in Tehran, Iran (2015-2016). Iranian J Neonatol 2018:9:49-56
Bordbar A, Mazouri A, Kashaki M, et al. Standard Multiple and Single Daily Dosing of Amikacin in Premature Infants. Iranian J Neonatol 2017 :8:57-64.
How to Cite
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.